The Columbia Disaster: Failures That Doomed The Space Shuttle

At 8:44 a.m. on February 1, 2003, Space Shuttle Columbia re-entered Earth's atmosphere at around 400,000 feet. Over the next eight minutes, Columbia descended 150,000 feet at Mach 24.1, causing extreme thermal heating and triggering the left wing sensors, which recorded greater strain than in previous Columbia re-entries.
As the orbiter cut through the skies above California and Nevada, superheated air blasted through a perforation in the craft's left wing that was the result of a debris strike during launch. The extreme temperatures melted the internal aluminum and warped the structure, causing serious aerodynamic imbalances.
Minutes later, in airspace southwest of Dallas-Fort Worth, Columbia's structure failed catastrophically and disintegrated at over 10,000 mph, killing the crew of seven. Tens of thousands of scraps and components rained across Texas, Arkansas and Louisiana. Only 38% — which still amounted to some 84,000 pieces — were recovered.
The tragedy occurred 17 years after the Challenger disaster in 1986, which the Rogers Commission attributed to flaws in design, management, and communication. Regrettably, the Columbia Accident Investigation Board (CAIB) established a similar range of institutional failings. The investigation revealed that NASA's organizational culture and decision making processes had not sufficiently improved, leading to the same oversight issues that caused the fatal foam strike on January 16, 2003. Here are the failures that doomed the Columbia space shuttle.
Foam debris strike and damage to thermal protection system
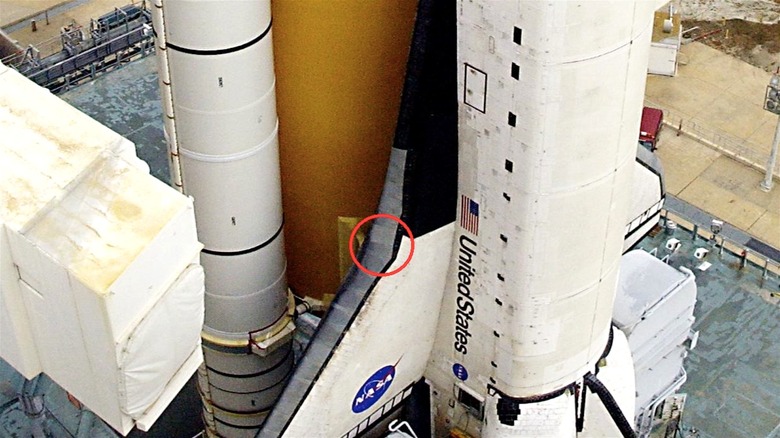
Like the rest of the space shuttle fleet, Columbia was attached to a 153-foot long external fuel tank with two umbilical fittings and a titanium bipod coated with low-density foam. This foam layer served dual purposes: insulating the cryogenic propellants inside the tank to maintain their low temperatures and reducing aerodynamic drag during the shuttle's ascent through the atmosphere.
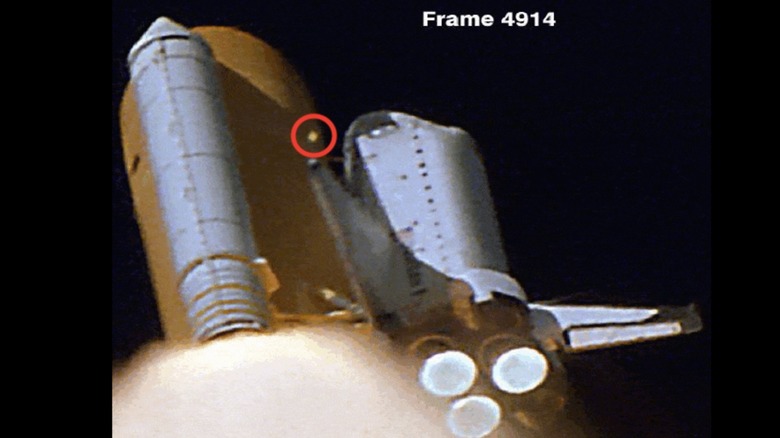
At 81.7 seconds into the launch, a large piece of this foam detached from the left external tank bipod and struck the Columbia's left wing 0.2 seconds later. The debris weighed only 1.67 pounds but it hit the wing at over 500 mph, damaging the reinforced carbon-carbon panels. The strike, which the crew members were informed in the following week, had no impact on the successful 16-day mission and remained of limited concern throughout the voyage.
Upon re-entry on February 1, the damaged panel allowed superheated air to rush into the thermal protection system and melt the interior. The first debris sightings occurred at 8:53 a.m. near the border of California and Nevada. Four more sightings occurred over the next 23 seconds and a further 18 sightings in the skies above Utah, Arizona, New Mexico and Texas. Mission Control lost contact with the Columbia at 8:59 a.m. and the orbiter disintegrated shortly thereafter.
Complacency regarding foam strikes
The Columbia Accident Investigation Board determined that institutional complacency led NASA operatives to express minimal concern about Columbia's foam strike, despite a design requirement that the external tank (ET) not shed foam or debris. It became clear that this requirement had not been fulfilled on Columbia's first launch in 1981, when debris shed the tank and destroyed over 300 heat-resistant tiles on the orbiter. This disturbed engineers who observed that even the light touch of one's thumbnail could dent parts of the thermal protection system.
However, foam strikes became so common that the Space Shuttle team grew to accept and even dismiss them, establishing a complacency that sociologist Diane Vaughan termed the "normalization of deviance," which refers to the pernicious acceptance of rule violations. The Columbia investigation established that foam strikes had occurred on every Space Shuttle launch to date and the board recommended that authorities launch an "aggressive program" to eliminate all debris shedding, especially around the bipod struts.
Foam continued to be an issue through the remainder of the Space Shuttle program. On July 26, 2005, NASA launched the STS-114 mission, its first since Columbia. Foam strikes were observed during launch and NASA grounded its fleet, but damage turned out to be minimal. Further strikes were suspected after the STS-135 launch, the last ever Space Shuttle mission, but these too were inconsequential.
Management, funding, and scheduling
The Columbia Accident Investigation Board's seven month investigation drew on the efforts and expertise of 13 board members, 120 board investigators, and thousands of NASA and support personnel. The board concluded that it was: "Convinced that the management practices overseeing the Space Shuttle Program were as much a cause of the accident as the foam that struck the left wing."
One of the first management issues concerned the film and photography crews tasked with recording the launch for engineering analysis. Two of the five crews failed to capture the foam strike at all, while the other three caught only a part of it. CAIB attributed the poor media performance to staff cuts, underfunding, and improper lens management.
Intense scheduling was also an issue. In fact, several NASA personnel contacted the CAIB investigation with complaints about the Space Shuttle's scheduling pressure. NASA employees spoke of how the date February 19, 2004 loomed large over NASA and the Space Shuttle program, for this was the intended launch date of STS-120 and the Node 2 component of the International Space Station. NASA had set this date with Congress in 2001 in an attempt to allay concerns about the complex ISS project, which was over budget and behind schedule. Pressure to meet this ambitious deadline caused persistent oversight.
Inadequate safety measures and communication

The Columbia Accident Investigation Board found numerous safety shortcomings with NASA's Space Shuttle program. For example, tests of the reinforced carbon-carbon system were deemed inadequate in measuring structural integrity, its supporting structure, and the attached hardware. The CAIB also found that the safety personnel were "present but passive" and did not challenge others effectively, weakening the program's safety culture. Some of the poorest communication occurred in the Mission Evaluation Room, where safety contractors were only minimally aware of the debris strike.
CAIB identified further faults in the Debris Assessment Team for its "stifled" decentralized decision-making process and limited communication with the Mission Management Team. However, the CAIB did note that problem-solving methods were extremely thorough in the Mission Control Center and Mission Management Team, indicating some areas of effective operation. Despite these positive aspects, the overall impact was compromised.
Ultimately, the report found that the Shuttle Program could not manage communication between the centralized and decentralized systems and even raised barriers that created "blind spots" in communication, compounding the complacency around foam strikes and other safety concerns.
Experimental design

In 1985, the Aerospace Safety and Advisory Panel warned NASA that the Space Shuttle was not an operational vehicle and should not be treated as such. The Challenger exploded the following year, affirming the panel's concerns. Despite this, NASA did not revise their perception of the orbiter through the next decade. In 1999, the Shuttle Independent Assessment Team doubled down on the 1985 report, reasserting the orbiter's experimental status. Despite these warnings, the Columbia Accident Investigation Board's 2003 report found that NASA had persisted in treating the orbiter as an operational vehicle rather than a "complex and risky" developmental vessel.
The CAIB explained NASA's outlook by pointing to the Space Shuttle program's record – there were 24 successful launches before the Challenger disaster and a further 87 successful launches through the rest of the 1980s, 1990s, and early 2000s. This, the CAIB reasoned, ingrained a level of success within NASA that caused leadership to overlook the experimental reality of the agency's technology. The board warned against the excessive "can-do" culture amongst engineers and called for an overhaul of the agency's technical safety practices, such as integrated hazard analysis and maintaining technical standards across all Space Shuttle Program projects.
Lack of effective real-time damage assessment

The Columbia Accident Investigation Board noted that Mission Control could not measure the foam strike damage to Columbia's wing. Once the Columbia was in mission, the Debris Assessment Team requested orbit images of the damaged wing. Their request was refused, however, and communication stalled with queries around the Debris Assessment Team's "mandatory need" for Department of Defense imaging.
Such obstruction was just another problem in NASA's questionable damage assessment infrastructure. CAIB found issue with the agency's use of the Crater model, a computer simulation tool designed to measure ice damage to the external tank. During Columbia's 16 days in orbit, engineers used Crater — which was essentially a piece of Apollo-era technology — to measure the foam strike damage. CAIB found notable fault with this procedure because the Crater model used particles some 400 times smaller than the foam chunk that struck Columbia's left wing, rendering the risk assessment data functionally useless.
The agency's failure to adopt more accurate and modern technologies for assessing damage directly contributed to the inability to address the foam strike's consequences adequately. In fact, NASA's preference for dated and irrelevant simulation over empirical, first hand analysis was among the greatest errors precluding the Columbia disaster.
Failure to develop contingency plans

The Columbia Accident Investigation Board accused managers of failing to develop a contingency plan to avoid a re-entry emergency. Space Shuttle leadership appeared to think that nothing could be done in an emergency, and no serious consideration was given to a rescue mission that could have retrieved the Columbia team or repaired the wing.
The CAIB asked NASA to theorize rescue and repair missions and they envisioned two scenarios. NASA underpinned the missions with the following narrative: On day one, debris strike discovered. The following day, mission managers would request imagery from Columbia crew. If the imagery proved inconclusive, then by day four NASA would ask the crew to perform a spacewalk to investigate damage. If the spacewalk reveals potentially catastrophic damage, then the crew would prepare and ration consumables. From day six to day 26 the shuttle program would work around the clock to mobilize, launch, and execute the mission.
NASA considered the repair mission to be "high risk" owing to the difficulty of the repair — a spacewalk with heavy components — and no guarantee that it would save the orbiter upon re-entry. A rescue mission had greater chances of success although not without serious challenges. In any event, these contingencies would have been preferable to what happened on February 1.
In their recommendations, CAIB posited a new agency-wide training program to develop contingency plans for emergency scenarios involving crew and shuttle loss.
Organization and wider working culture

In a highly critical summary, the Columbia Accident Investigation Board accused NASA of addressing none of the issues that caused the 1986 Challenger disaster. The agency's shift towards a more business-like mentality, with an emphasis on "faster, better, cheaper," was identified as detrimental to maintaining the high standards of safety required for human spaceflight. This created significant potential for catastrophic issues "with schedules, production pressures, deadlines, and cost efficiency goals elevated to the level of technical innovation and safety goals," the report read.
CAIB identified NASA's extreme "can-do" culture as a dangerous feature of both the Challenger and Columbia disasters. The agency's unyielding optimism caused it to dismiss safety concerns, overlook the Orbiter's experimental nature, and pursue harried schedules. Furthermore, the CAIB observed a marked cultural shift in the organization that valued hierarchy and bureaucracy rather than the engineering expertise that steered the Apollo program to success in the 1960s. These patterns created a brew of austerity, bureaucracy, complacency and ignorance that proved fatal for the seven astronauts on February 1, 2003.
CAIB made a raft of recommendations, including the establishment of a Technical Engineering Authority responsible for monitoring and enforcing safety standards with waiver-holding authority. CAIB also advised a restructure of the Space Shuttle Integration Office so that it was capable of truly integrating all teams within the program.